 Joan Tur, of Clarivate Analytics, attended February’s EACR Virtual Conference, Defence is the Best Attack: Immuno-Oncology Breakthroughs. Below you can read his report about the meeting, and the science that was covered. You can also read the EACR’s summary here.
Joan Tur, of Clarivate Analytics, attended February’s EACR Virtual Conference, Defence is the Best Attack: Immuno-Oncology Breakthroughs. Below you can read his report about the meeting, and the science that was covered. You can also read the EACR’s summary here.
Following two highly successful editions and a cancellation in 2020 due to the COVID-19 pandemic, the European Association for Cancer Research (EACR) resumes its ‘Defence is the Best Attack: Immuno-Oncology Breakthroughs’ conference in 2021 with its third edition as a worldwide virtual event. The meeting covered the latest advances in the field of immuno-oncology, ranging from preclinical research to pre-and post-marketing studies. The covered topics included identification of new actionable targets, use of precision medicine as a tool to improve response rates to current treatments, and modulation of the tumor microenvironment (TMI) to promote anticancer immune responses.
CSF CTDNA as a Non-Invasive Biomarker to Predict Brain Metastasis Responses to Immunotherapy
Immunotherapy, and in particular immune checkpoint inhibitors, have demonstrated robust and durable responses in many advanced or metastatic solid tumors, including in brain metastasis; however, brain metastasis tends to show a worse response to immune checkpoint inhibitors compared with the extracranial lesions from which they originate (most frequently melanoma or lung cancer), and only a small fraction of such patients respond to these therapies, highlighting the need for therapy predictive biomarkers. These differential responses are explained in part by the composition of TMI, particularly its immune cell composition, whose characterization is emerging as a powerful tool in precision medicine to select the treatments that are most likely to help patients based on their individual characteristics, as well as to discover new actionable targets to improve the efficacy of existing immunotherapies.
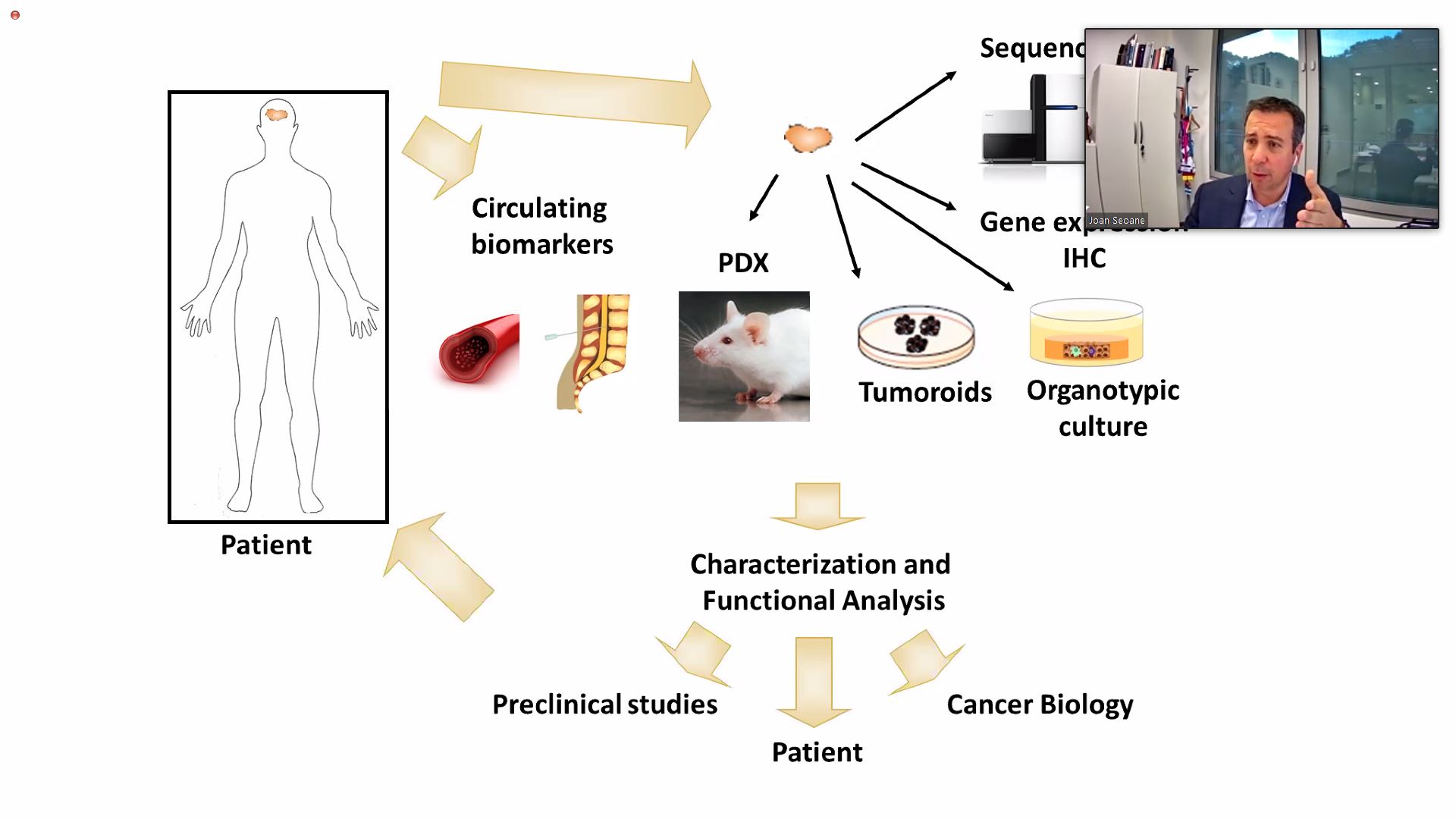
Due to the very nature of its location, obtaining representative biopsies from brain metastasis is a highly invasive and challenging surgery procedure. Joan Seoane (Vall d’Hebron Institut d’Oncologia (VHIO)/Mosaic Biomedicals) presented a relatively safer and less-invasive approach using the circulating tumor DNA (ctDNA) found in the CSF as a liquid biopsy. ctDNA is shed from cells in the tumor and can provide fundamental information about the immune cell landscape in the TMI (eg, infiltration of T cells, activation of pro-inflammatory phenotype in macrophages, proliferation of NK cells). All this information allows making predictions about the potential benefit of immunotherapies (eg, if there is no lymphocyte infiltration it is very unlikely that immune checkpoint inhibitors will work) and allows for monitoring patients in real time to evaluate their responses to a particular therapy, being able to rapidly switch to another if there is no response to the first one.

Finally, the information provided by CSF ctDNA can be used as a powerful tool in the discovery of potentially druggable targets. One example is leukemia inhibitory factor (LIF), a protein produced by macrophages and dendritic cells in the TMI, that was shown to prevent CD8+ T-cell tumor infiltration, impairing the response to immune checkpoint inhibition. Dr Seoane briefly mentioned that his group (through the spin-off company Mosaic Biomedicals) was the originator of MSC-1, an anti-LIF antibody currently in clinical development by Northern Biologics and Bristol-Myers Squibb, and that it has already shown very promising phase I data; following a summary of already published data from the MSC-1-101 phase I study it was announced that a phase II study is expected to begin later this year.
Downregulation of JAK2 Promotes Acquired Tumor Resistance to Anti-HER2 Bispecfic Antibodies and CAR T-Cell Therapies
It is usually assumed that the main obstacle preventing the response to cancer immunotherapies is the lack of active cytotoxic T cells within the tumor (either because they are not recruited or because they fail to become activated); however, even with active cytotoxic T-cell infiltration, tumors can acquire resistance to avoid being killed. Enrique Javier Arenas Lahuerta (VHIO) and Christian Klein (Roche) presented a study showing that downregulation of the kinase JAK2, which transduces the signal initiated by IFN-gamma, is the preferred widespread strategy used by cancer cells to resist clearance by directed lymphocytes.
Murine models of resistant tumors were injected with either a HER2/CD3 bispecific T-cell engager or an anti-HER2 CAR T-cell therapy. As expected, tumor volume was significantly increased in resistant mice compared with their wild-type counterparts: wild-type animals showed an increase in IFNgamma-related gene signatures. When the expression of IFN-gamma was suppressed in the wild-type mice (via CRISPR-Cas9), these acquired resistance to immunotherapy, as shown by the increased tumor burden, demonstrating that IFN-gamma signaling is required for efficient killing by lymphocytes. When evaluating which component of the IFN-gamma pathways was affected, only JAK2 was shown to be downregulated in the resistant animals. The central role of JAK2 downregulation in the acquisition of resistance was confirmed when resistant animals in which JAK2 expression had been restored lost their resistant phenotype. These results support using JAK2 and IFN-gamma as surrogate biomarkers to predict response to bispecific T-cell engagers and CAR T-cell therapies, as well as the potential use of drugs targeting JAK2 to make the tumors susceptible to immunotherapies again.
Oncolytic Measles Virus Therapy with CD47 Blockade Promotes Tumor Cell Phagocytosis by Macrophages
CD47 is an immunoglobulin that is overexpressed on the surface of many cancer cells. This molecule interacts with SIRP-alpha, enabling the escape of cancer cells from macrophage-mediated phagocytosis. Lukas Kuchernig (German Cancer Research Center) presented a strategy to overcome this issue by using oncolytic measles virus (MeVac) expressing a blocking antibody against CD47 (MeVac H-aCD47). The aim of this therapy is to promote anticancer responses via dual mechanism of action: on one hand the oncolytic virus would selectively spread in the tumor tissue leading to lysis of tumor cells, release of damage-associated molecular patterns (DAMPs), and recruitment and activation of the immune system (including macrophages); on the other hand, CD47 blockade would promote phagocytosis by the macrophages that have just been recruited and activated.
The product demonstrated cytotoxicity against human ovarian carcinoma cells in vitro, as well as the production of anti-CD47 that specifically and effectively bound to CD47. When the infected carcinoma cells were co-cultured with macrophages, these macrophages became activated to an M1-like polarized phenotype (ie, pro-inflammatory and anticancer phenotype) and showed increased phagocytosis against these tumor cells. It was announced that, following a few more in vitro assays using CD47 knock-out cell lines, Mr Kuchernig’s group intends to begin in vivo studies to test the efficacy of MeVac H-aCD47.
Eosinophils and Tregs as Potential New Targets for Breast Cancer Metastasis
In the majority of cases, breast cancer mortality is the result of tumor metastasis, with lymph nodes and the lung normally being the first sites where the cancer spreads. Two consecutive presentations highlighted the role two types of different kinds of immune cell, eosinophils and regulatory T cells (Tregs), respectively, in determining the evolution of these metastases, as well as conditioning their susceptibility to immuno-oncology treatments.

Sharon Grisaru (Tel Aviv University) highlighted the importance of the anti-cancer activities of eosinophils, a type of immune cell normally associated with allergic reactions but is also present in 95% of lung cancer metastases from breast cancer patients. These cells are actively recruited to the lung metastases, as demonstrated in a mouse model of breast cancer lung metastasis, showing a rapid homing of eosinophils to the lung via a CCR3-independent pathway. The antitumorigenic activities of eosinophils was confirmed by their depletion, either via anti-Siglec-F antibody or using KO mice, resulting in an increase of the tumor burden. This anticancer activity was not performed directly by the eosinophils themselves, whose main involvement was shown to be the recruitment of CD8-positive T cells to the TMI via CXCL9/10 pathways. To initiate the recruitment of cytotoxic T cells, eosinophils also first needed to become activated by a series of factors in the TMI, including IFNgamma and TNF-alpha; therefore, the modulation of eosinophil activity, either directly or by changing the composition of activating factor in the TMI, is emerging an actionable target for the development of new immuno-oncology therapies to prevent breast cancer lung metastasis.

An alternative strategy to activate cells that promote antitumor responses is to inhibit cells in the TMI that promote tumor function. Kevin Kos (Netherlands Cancer Institute) focused on the pro-tumorigenic effect of Tregs in driving breast cancer lymph node metastasis. Mammary tumor development leads to a systemic increase of activated Tregs, as demonstrated in a mouse model of spontaneous breast cancer (KEP), which showed not only an increase in Tregs, but also an increase in activation (as shown by an increased expression of the immunosuppressive markers CTLA4 and ICOS), suggesting that the tumor is recruiting and educating Tregs to defend itself against the immune system attacks, particularly from T cells and NK cells. These overactivated Tregs accumulate in the mammary gland, but also in lung and lymph node metastases that arise in the KEP-based metastasis model. Depletion of Tregs (via FoxP3 antibody) significantly reduced metastasis to axillary lymph nodes, but strikingly it did not show any effect in lungs. It was hypothesized that the reliance of Treg modulation to prevent attacks from the immune system may be tissue-dependent, being essential to generate metastases in the lymph nodes but almost irrelevant in the lungs.
Myc Inhibition via Omomyc-Based Therapy Shows Potential to Interfere with Tumor Immune Evasion
Omomyc (OMO-103) is a cell-penetrating peptide therapeutic that, once inside the cell, dimerizes with the Myc oncoprotein, inhibiting its function. The therapy is currently being investigated by Peptomyc and Syros Pharmaceuticals for the potential iv or intranasal treatment of cancer and has already demonstrated preliminary efficacy in multiple preclinical models.
Sílvia Casacuberta-Serra from Peptomyc presented further preclinical data demonstrating for the first time that, in addition to its direct effect in preventing tumor proliferation and promoting apoptosis, Omomyc also promotes intratumor immune cell recruitment. In a mouse model of KRASG12D-driven NSCLC adenocarcinoma intranasal Omomyc significantly reduced tumor burden. The therapy changed the cytokine/chemokine signature and promoted the recruitment and expansion of immune cells to the tumor site, including CD4+ T cells (particularly Th17 and Th1 cells), CD8+ T cells and dendritic cells. Both types of T cells showed higher levels of activation were more reactive to the tumor (as shown by the expression of PD-1 and Tim-3) and showed increased proportions of effector/memory phenotype. Similar data were observed in several mouse models of NSCLC regardless of their driving mutations, including KRAS, p53 or EGFR, confirming that the immunostimulatory effect is not dependent on the tumor mutational profile.
Immunotherapy Combinations to Improve the Outcomes in Ovarian Cancer
A topic extensively covered at this conference was the importance of immunotherapy combinations to improve outcomes in cancer patients. Kunle Odunsi (Roswell Park Comprehensive Cancer Center) focused his talk on immune checkpoint combinations in ovarian cancer, highlighting different strategies that have demonstrated initial success, and showing a glimpse into the future of immunotherapy combinations for ovarian cancer.

Immune checkpoint inhibitors have shown promise in ovarian cancer, but their effectiveness is limited by multiple immune suppressive networks in the TME, including compensatory increases in checkpoint expression when another is inhibited, activation of suppressive cells (Tregs, myeloidderived suppressor cells and tolerogenic dendritic cells), soluble factors (cytokines such as TGF-beta, and chemokines such as CXC4/CXCL12) and energy/metabolic mechanisms (eg, arginine starvation).
To be successful and avoid these suppressive mechanisms, an immunotherapy combination needs to fulfill three requirements: deliver large numbers of T cells to the TMI (eg, checkpoint inhibitor in combination with adoptive T-cell therapy or vaccination), counteract innate and adaptive mechanisms of immune resistance (eg, combination of multiple checkpoint inhibitors to prevent compensatory mechanisms, combination of checkpoint inhibitors and Treg modulators) and be personalized based on individual’s tumor immune landscape (eg, biomarker evaluation to predict response to combination therapy while minimizing toxicities).